Arthroscopic Shoulder Stabilisation
Arthroscopic Shoulder Stabilisation
Post Op Protocol
The Operative Notes should accompany you on discharge in a folder with other documents including your physio referral. PLEASE give this information to the physio to individualise your rehab.
Also NOTE if a BICEPS TENODESIS was performed!!
Day 1 to day 7
– In hospital ICE / cryo-cuff every 2-3 hours
– Do not put up with pain!! Ensure you take adequate pain relief
– You may need to seeyour GP for additional medication or contact Dr Maguire’s Rooms
– If no contraindications use this pain relief regime
– PCA overnight then change to the following in am:
– Paracetamol 1gram four times a day
– Ibuprofen 400mg three times a day
– 10 to 20 mg of TARGIN (Oxycontin) twice a day
– 5-10 mg of Endone as required up to 3 hourly
– Ensure Fluid intake and bowel softening agents
– Prevent constipation from Endone/Targin
– Remain in sling unless doing physio or showering or if doing simple activity
– MUST wear sling to bed!!!
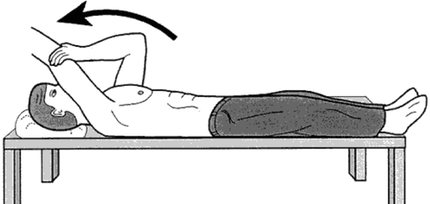
– Gentle pendulum exercises
(Forwards/Backwards)(Left/Right)
– Hand, wrist, elbow ROM (Range of Motion) as tolerated
– External rotation to neutral (0 Degrees only)
– Protect Biceps if Tenodesis performed
– Support Elbow
– No active contraction of biceps
– Scapula exercises (shrugs, protaction, retraction, rolls)
– As frequently as tolerated
– Maintain cardiovascular exercise after Day 3 may start walking, stationary bike
Weeks 2 to 6
– Continue exercises above
– Wean off Targin and Endone after first week. (Try to stop Targin after a few days and just take Endone when needed)
– Continue Panadol and Neurofen if no contraindications (Ask GP if not sure)
– Abduction sling on unless showering, eating or sitting
– Sling ALWAYS on for sleeping and when mobilising
– Remain in sling unless doing physio or showering or if doing simple activity
– MUST wear sling to bed!!!
– Gentle Pendular movements (Assisted)
– PROM (Passive Range of Motion) only!
– PROM Supine FE gently up to 140 (only 10 reps max)
– Table slides into FE as tolerated (only 10 reps max)
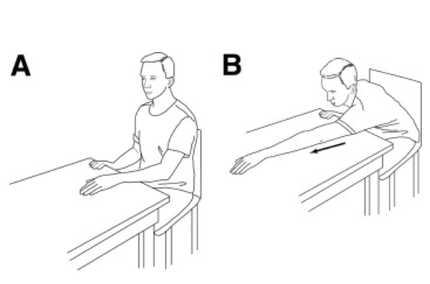
Figure 1. Table slide. (A) Starting position. While seated at a table, the patient places the hand of the affected shoulder on a sliding surface (e.g., a magazine that slides over a smooth table surface). (B) Ending position. The patient slides the hand forward, maintaining contact with the table, while the head and chest advance toward the table.
– External Rotation (ER) to 30 degrees (only 10 reps max)
– If large subscapularis tear ER to neutral till wk 6
– Internal rotation to buttock (only 10 reps max)
– Warm-up before exercises
– Walk for 1 minutes
– Warmth to shoulder (warm pack or warm shower)
– ICE after exercises for 30 mins
– Gentle isometric contractions of Rotator Cuff

– Start gentle theraband work if no rotator cuff repair
– Use core muscle exercises and lower limb exercises from Day 1 post Op
– e.g. Kibler Kinetic Chain Theory
– Protect Biceps if Tenodesis performed
– Support Elbow
– No active contraction of biceps
– Aerobic exercise (walking or stationary exercise bike)
Weeks 7 to 8
– Continue above exercises
– Discontinue sling after 6 wks and perform normal ADL’s (Activities of Daily Living)
– Begin Assisted AROM at 7wks (Unless Rotator Cuff Tear)
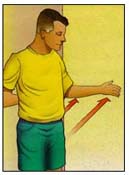
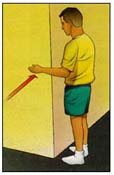
– Assisted AROM includes “wall walking” for FE

– Push PROM to achieve FROM (Full Range of Motion)
– Start gentle theraband work 2 wks after Assisted AROM
– Only for cuff muscles not repaired
– e.g. Medium Tear at 10 wks
– Continue theraband work if no rotator cuff repair
– Continue cardiovascular conditioning
– Continue hand, wrist, elbow exercises
– Core strengthening especially transversus abdominis, multifidus
– Scapular mobilization / proprioception
– Avoid full abduction and external rotation as this may disrupt repair
Weeks 9 to 12
– Continue above exercises
– Begin Gym program
– May start running and pool work
– Progress from gentle breastroke to freestyle
– Avoid heavy lifting for 3 months
– Lift with arms close to body
– This avoids the “Lever Arm Effect”
– If significant stiffness or pain at 12 wks may consider corticosteroid injection
At 3 months
– Start capsular stretches
– Continue cuff strengthening
– Start formal gym program
– Advance cardiovascular conditioning
– Core strengthening
– Continue scapular mobilization / proprioception
– May consider return to contact sport or heavy manula labour at 4 months in shoulder brace


– Most patients return to sport at 6+ months
6 months to 12 months
– If stiffness persists for 12 months may consider arthroscopic capsular release